Salome Baya had only been working at the Coast General Provincial and Referral Hospital for a month. While cleaning the labor ward, she picked up a stack of papers from the floor and felt something prick her finger.
“I knew it was a needle,” she recalls. “It got stuck on my finger. I flushed my finger under running water before going to see a doctor, who examined my hand and gave me a PEP.”
A facility like Coast General produces 60–80 kilograms of infectious and highly infectious waste every day. If not properly disposed of, this waste presents a serious danger to people who come in contact with it. It can harbor chemical contaminants or become a breeding ground for infectious microbes.
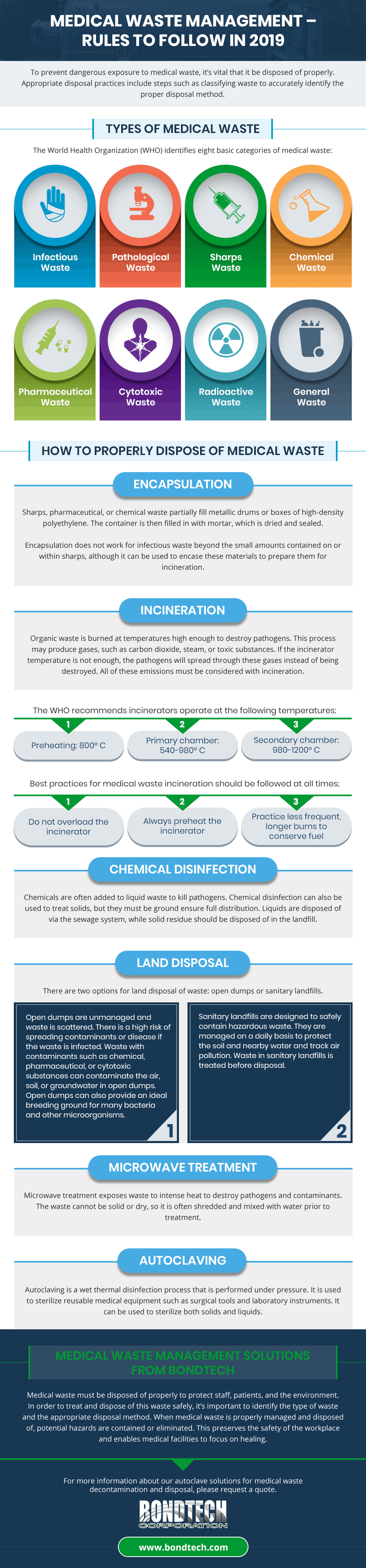
To prevent dangerous exposure to medical waste, it’s vital that it be disposed of properly. Appropriate disposal practices include steps such as classifying waste to accurately identify the proper disposal method.
This guide will walk you through the process of proper medical waste management. We’ve provided a checklist to ensure you have everything you need to dispose of hospital waste properly.
Types of Medical Waste
The World Health Organization (WHO) identifies eight basic categories of medical waste:
- Infectious waste such as bandages, swabs, and disposable medical devices from infected patients; or waste with body fluids such as cultures, infectious agents, or diagnostic samples used by laboratories.
- Pathological waste refers to body parts, tissue, organs, and fluids from humans or animals.
- Sharps waste such as needles, scalpels, blades, and syringes.
- Chemical waste from chemicals used in laboratories, such as reagents, solvents, and disinfectants. This category also includes heavy metals from batteries or medical devices, such as mercury from a broken thermometer.
- Pharmaceutical waste includes vaccines and drugs that are expired, unused, or contaminated.
- Cytotoxic waste contains substances that are carcinogenic, mutagenic, and teratogenic—for example, the cytotoxic drugs used for treating cancer.
- Radioactive waste refers toa variety of waste used in diagnostics or disease treatments, such as radioactive diagnostic agents and radio-therapeutic agents.
- General waste categorizes general waste that doesn’t pose any risks.

A street boy picks a piece of biomedical waste; syringes, needles, drugs and other medical waste, that was found at Nyeri dumpsite on August 18, 2014. PHOTO | JOSEPH KANYI
How to Properly Dispose of Medical Waste
There are a variety of ways to handle medical waste. The appropriate disposal method depends on the type of waste and the risks it poses. The most common methods include:
Encapsulation
Sharps, pharmaceutical, or chemical waste partially fill metallic drums or boxes of high-density polyethylene. The container is then filled in with mortar, which is dried and sealed.
Encapsulation does not work for infectious waste beyond the small amounts contained on or within sharps, although it can be used to encase these materials to prepare them for incineration.
Incineration
Organic waste is burned at temperatures high enough to destroy pathogens. This process may produce gases, such as carbon dioxide, steam, or toxic substances. If the incinerator temperature is not enough, the pathogens will spread through these gases instead of being destroyed. All of these emissions must be considered with incineration.
The WHO recommends incinerators operate at the following temperatures:
- Preheating: 800° C
- Primary chamber: 540-980° C
- Secondary chamber: 980-1200° C
Best practices for medical waste incineration should be followed at all times:
- Do not overload the incinerator
- Always preheat the incinerator
- Practice less frequent, longer burns to conserve fuel

Bondtech Corporation Field Service Manager David Cavanaugh yesterday explains how the newly acquired shredder machine works ahead of their commissioning of Friday. PHOTO | BRIAN WACHIRA
Chemical Disinfection
Chemicals are often added to liquid waste to kill pathogens. Chemical disinfection can also be used to treat solids, but they must be ground ensure full distribution. Liquids are disposed of via the sewage system, while solid residue should be disposed of in the landfill.
Land Disposal
There are two options for land disposal of waste: open dumps or sanitary landfills.
- Open dumps are unmanaged and waste is scattered. There is a high risk of spreading contaminants or disease if the waste is infected. Waste with contaminants such as chemical, pharmaceutical, or cytotoxic substances can contaminate the air, soil, or groundwater in open dumps. Open dumps can also provide an ideal breeding ground for many bacteria and other microorganisms.
- Sanitary landfills are designed to safely contain hazardous waste. They are managed on a daily basis to protect the soil and nearby water and track air pollution. Waste in sanitary landfills is treated before disposal.
Microwave Treatment
Microwave treatment exposes waste to intense heat to destroy pathogens and contaminants. The waste cannot be solid or dry, so it is often shredded and mixed with water prior to treatment.
Autoclaving
Autoclaving is a wet thermal disinfection process that is performed under pressure. It is used to sterilize reusable medical equipment such as surgical tools and laboratory instruments. It can be used to sterilize both solids and liquids.
When to Use an Autoclave
Autoclaves are increasingly being considered as a viable substitute for incineration because they eliminate the emissions caused by burning waste. They do not use chemicals and are able to treat a majority of the infectious waste produced in medical settings. Autoclave treatment destroys microbes to make medical waste safe for disposal in open landfills.
Of note, autoclaves cannot be used to treat hazardous waste, such as chemotherapy drugs, certain expired medications, and cytotoxic materials. The temperature is too low to destroy these toxins, and the process can aerosolize them.
At Bondtech Corp. we provide durable high-vacuum and high-pressure autoclave systems to sterilize infectious waste, including biomedical waste. Our autoclaves are controlled by programmable logic controllers (PLC) and feature our proprietary, quick-opening door and high vacuum system.
Medical Waste Management Solutions from Bondtech
Medical waste must be disposed of properly to protect staff, patients, and the environment. In order to treat and dispose of this waste safely, it’s important to identify the type of waste and the appropriate disposal method. When medical waste is properly managed and disposed of, potential hazards are contained or eliminated. This preserves the safety of the workplace and enables medical facilities to focus on healing.
For more information about our autoclave solutions for medical waste decontamination and disposal, please request a quote.